PITUITARY ADENOMAS
Pituitary adenomas are non-cancerous tumors that develop in the pituitary gland, a small, pea-sized gland located at the base of the brain. Despite being benign, these tumors can cause significant health issues due to their location and the hormones they can produce or disrupt. The pituitary gland plays a crucial role in regulating various hormones that control growth, metabolism, reproduction, stress response, and other bodily functions.
Pituitary adenomas can be classified based on the hormones they secrete or their size. They are categorized as:
-
Functioning Adenomas: These tumors produce excessive amounts of hormones, leading to hormonal imbalances. Common types include prolactinomas (overproduction of prolactin), somatotropinomas (excessive growth hormone), corticotropinomas (overproduction of ACTH leading to Cushing’s disease), and thyrotropinomas (excess thyroid-stimulating hormone).
-
Non-Functioning Adenomas: These tumors do not produce significant amounts of hormones but can cause symptoms due to their size and compression of nearby structures.
Pituitary adenomas can be further classified based on their size into two main categories: microadenomas and macroadenomas. These classifications refer to the diameter of the tumor.
-
Microadenomas: Microadenomas are small pituitary adenomas, usually measuring less than 1 centimeter in diameter. Despite their small size, they can still cause significant hormonal imbalances due to their location within the pituitary gland. Microadenomas often present with symptoms related to hormone overproduction (functional microadenomas) or due to compression of nearby structures (non-functioning microadenomas).
-
Macroadenomas: Macroadenomas are larger pituitary adenomas, typically measuring 1 centimeter or more in diameter. Because of their size, macroadenomas can cause symptoms related to compression of nearby structures, such as the optic nerves, leading to visual disturbances. Like microadenomas, macroadenomas can also be functioning (producing excess hormones) or non-functioning (not producing significant hormones).
Symptoms of pituitary adenomas vary based on the type and size of the tumor. They may include hormonal imbalances, visual disturbances, headaches, fatigue, menstrual irregularities, growth abnormalities, and more. The diagnosis involves medical imaging, hormone level tests, and often consultation with endocrinologists and neurosurgeons.
Treatment options depend on factors such as tumor size, hormone production, and patient health. They can include medication, surgery to remove the tumor, radiation therapy, or a combination of these approaches. Pituitary adenomas are generally treatable, and early diagnosis and appropriate management can lead to improved outcomes.
MRI APPEARANCE
Pituitary adenomas can be characterized on MRI scans by their T1-weighted, T2-weighted, and post-contrast T1-weighted appearances. Here’s a general overview of how they might appear:
-
T1-weighted Imaging (T1WI): Pituitary adenomas typically appear as iso- to mildly hypointense compared to gray matter due to their solid nature. This is due to the relatively higher fat content and variable protein content in these tumors.
-
T2-weighted Imaging (T2WI): Pituitary adenomas usually appear hyperintense on T2WI due to their high water content. The signal intensity can vary based on the tumor’s consistency and cystic components.
-
Post-Contrast T1-weighted Imaging: After contrast administration (usually gadolinium-based contrast agents), pituitary adenomas can enhance. The degree and pattern of enhancement can vary, with some adenomas showing homogeneous enhancement while others might have areas of heterogeneous enhancement or rim enhancement.
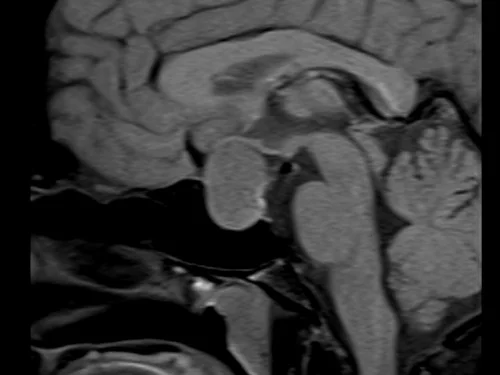
T1 SAGITTAL PRE CONTRAST

T1 CORONAL PRE CONTRAST

T2 CORONAL

T1 SAGITTAL POST CONTRAST

T1 CORONAL POST CONTRAST
REFERENCES
- Osborn, A. G., Preece, M. T. (2006). Intracranial tumors and masses: Radiology-Pathology Correlations from Head to Toe. Amirsys, Inc.
- Lee, D. K., & Lee, K. S. (2015). Magnetic resonance imaging of pituitary adenomas. Quantitative Imaging in Medicine and Surgery, 5(4), 576–591.
- Trouillas, J., & Jaffrain-Rea, M. L. (2009). Pituitary adenomas and related disorders. Springer.
- Barkhoudarian, G., & Kelly, D. F. (2011). Pituitary adenomas: Historical perspective, surgical management and future directions. CNS Oncology, 1(1), 29–41.
- Laws Jr, E. R., & Lopes, M. B. (2010). Pituitary tumors. Diagnostic pathology: Neuropathology. Amirsys.
U tuyến yên là khối u không phải ung thư phát triển trong tuyến yên, một tuyến nhỏ có kích thước bằng hạt đậu nằm ở đáy não. Mặc dù lành tính nhưng những khối u này có thể gây ra các vấn đề sức khỏe nghiêm trọng do vị trí của chúng và các hormone mà chúng có thể sản xuất hoặc phá vỡ. Tuyến yên đóng một vai trò quan trọng trong việc điều chỉnh các loại hormone khác nhau kiểm soát sự tăng trưởng, trao đổi chất, sinh sản, phản ứng căng thẳng và các chức năng cơ thể khác.
U tuyến yên có thể được phân loại dựa trên hormone chúng tiết ra hoặc kích thước của chúng. Chúng được phân loại là:
-
U tuyến chức năng: Những khối u này tạo ra lượng hormone quá mức, dẫn đến mất cân bằng nội tiết tố. Các loại phổ biến bao gồm u tiết prolactin (sản xuất quá mức prolactin), u somatotropinomas (hormone tăng trưởng quá mức), u corticotropinomas (sản xuất quá mức ACTH dẫn đến bệnh Cushing) và u tuyến giáp (thừa thừa hormone kích thích tuyến giáp).
-
U tuyến không hoạt động: Những khối u này không sản xuất ra lượng hormone đáng kể nhưng có thể gây ra các triệu chứng do kích thước của chúng và sự chèn ép của các cấu trúc gần đó.
U tuyến yên có thể được phân loại thêm dựa trên kích thước của chúng thành hai loại chính: u tuyến nhỏ và u tuyến lớn. Những phân loại này đề cập đến đường kính của khối u.
-
U tuyến nhỏ: U tuyến nhỏ là u tuyến yên nhỏ, thường có đường kính dưới 1 cm. Mặc dù có kích thước nhỏ nhưng chúng vẫn có thể gây mất cân bằng nội tiết tố đáng kể do vị trí của chúng trong tuyến yên. Các u tuyến nhỏ thường xuất hiện với các triệu chứng liên quan đến việc sản xuất quá mức hormone (các u tuyến nhỏ chức năng) hoặc do sự chèn ép của các cấu trúc lân cận (các u tuyến nhỏ không hoạt động).
-
Macroadenomas: Macroadenomas là u tuyến yên lớn hơn, thường có đường kính từ 1 cm trở lên. Do kích thước của chúng, u tuyến lớn có thể gây ra các triệu chứng liên quan đến chèn ép các cấu trúc gần đó, chẳng hạn như dây thần kinh thị giác, dẫn đến rối loạn thị giác. Giống như u tuyến nhỏ, u tuyến lớn cũng có thể hoạt động (sản xuất hormone dư thừa) hoặc không hoạt động (không sản xuất hormone đáng kể).
Các triệu chứng của u tuyến yên khác nhau tùy thuộc vào loại và kích thước của khối u. Chúng có thể bao gồm mất cân bằng nội tiết tố, rối loạn thị giác, đau đầu, mệt mỏi, kinh nguyệt không đều, tăng trưởng bất thường, v.v. Việc chẩn đoán bao gồm hình ảnh y tế, xét nghiệm mức độ hormone và thường tham khảo ý kiến của bác sĩ nội tiết và bác sĩ phẫu thuật thần kinh.
Lựa chọn điều trị phụ thuộc vào các yếu tố như kích thước khối u, sản xuất hormone và sức khỏe bệnh nhân. Chúng có thể bao gồm dùng thuốc, phẫu thuật để loại bỏ khối u, xạ trị hoặc kết hợp các phương pháp này. U tuyến yên thường có thể điều trị được, chẩn đoán sớm và điều trị thích hợp có thể dẫn đến kết quả được cải thiện.
XUẤT HIỆN MRI
U tuyến yên có thể được đặc trưng trên chụp MRI bằng hình ảnh T1W, T2W và sau tương phản. Dưới đây là tổng quan chung về cách chúng có thể xuất hiện:
-
Hình ảnh T1W (T1WI): U tuyến yên thường xuất hiện dưới dạng giảm tín hiệu từ đồng mức đến nhẹ so với chất xám do tính chất rắn của chúng. Điều này là do hàm lượng chất béo tương đối cao hơn và hàm lượng protein thay đổi trong những khối u này.
-
Hình ảnh T2W (T2WI): U tuyến yên thường xuất hiện tăng tín hiệu trên T2WI do hàm lượng nước cao. Cường độ tín hiệu có thể thay đổi dựa trên tính nhất quán và thành phần nang của khối u.
-
Hình ảnh T1W sau tiêm thuốc cản quang: Sau khi dùng thuốc cản quang (thường là thuốc cản quang gốc gadolinium), u tuyến yên có thể ngấm thuốc. Mức độ và kiểu bắt thuốc có thể khác nhau, với một số u tuyến cho thấy bắt thuốc đồng nhất trong khi những u khác có thể có các vùng bắt thuốc không đồng nhất hoặc bắt thuốc ở viền.
T1 SAGITTAL TRƯỚC TƯƠNG PHÁP
T1 CORONAL TRƯỚC TƯƠNG LAI
T2 CORONAL
T1 SAGITTAL SAU TƯƠNG PHƯƠNG
T1 CORONAL SAU TƯƠNG PHƯƠNG
NGƯỜI GIỚI THIỆU
- Osborn, AG, Preece, MT (2006). Các khối u và khối nội sọ: Mối tương quan X quang-Bệnh học từ đầu đến chân. Amirsys, Inc.
- Lee, DK, & Lee, KS (2015). Hình ảnh cộng hưởng từ của u tuyến yên. Hình ảnh Định lượng trong Y học và Phẫu thuật, 5(4), 576–591.
- Trouillas, J., & Jaffrain-Rea, ML (2009). U tuyến yên và các rối loạn liên quan. Mùa xuân.
- Barkhoudarian, G., & Kelly, DF (2011). U tuyến yên: Quan điểm lịch sử, quản lý phẫu thuật và hướng đi trong tương lai. Ung thư CNS, 1(1), 29–41.
- Laws Jr, ER, & Lopes, MB (2010). Các khối u tuyến yên. Bệnh lý chẩn đoán: Bệnh lý thần kinh. Amirsys.